

Introduction
Let’s talk biopsies!
Biopsies are a hot topic in the lichen sclerosus community. Some of us have had one (or more); some of us haven’t had one. In today’s post, I’m going to talk about biopsy basics for lichen sclerosus. Specifically, I am going to address the two ways lichen sclerosus is diagnosed, when a biopsy is necessary, and what this procedure involves. In my next post, I will share a bunch of important biopsy tips for before, during, and after the procedure. Be sure to subscribe to TLLC’s newsletter so you don’t miss that post!
*Please note: When referring to lichen sclerosus diagnosis and biopsies in this post, I am referring to vulvar lichen sclerosus and vulvar biopsies. This information does not pertain to penile lichen sclerosus.
How is Lichen Sclerosus Diagnosed?
Let’s start with the basics – how is lichen sclerosus diagnosed?
Lichen sclerosus is diagnosed in one of two ways:
- Clinical examination
- Vulvar biopsy
Clinical Examination: What You Need to Know
A clinical diagnosis involves two components: symptoms (what you feel) and signs (what you see). Let’s go over each.
Lichen Sclerosus Symptoms
- Itch, which may be mild to severe
- Pain (e.g., burning, stinging)
- Dyspeurenia (i.e., pain with sex)
- Tearing during sex or physical activity
- Fissures and cuts (e.g., stinging and sharp pain-like sensations)
- Difficulty urinating or defecating
- Asymptomatic (i.e., some patients with lichen sclerosus have signs but no symptoms)
Lichen Sclerosus Signs
- Changes in skin pigmentation (most commonly whiteness or white patches/plaques on the vulva)
- Swelling (often from chronically scratching the area)
- Bruising (often from chronically scratching the area)
- Changes to the texture of the skin (e.g., it can look waxy, shiny, and may in some cases appear thin). However, it’s important to note lichen sclerosus doesn’t thin the skin; instead, it thickens the skin below the top layer of the skin, and this thickening leads to other signs such as fissures and fusing. To learn more, check out my YouTube video on does LS thin or thicken the skin here.
- Fissures (i.e., splitting of the skin)
- Fusing (i.e., when different parts of the vulva stick to each other that are not supposed to)
- Resorption (i.e., when different parts of the vulva resorb into the surrounding vulvar anatomy). *See my YouTube video on lichen sclerosus terminology to learn more about fusing and resorption here.
Back to the Clinical Diagnosis
To make a clinical diagnosis, your healthcare provider will start by taking a detailed history of your symptoms. For example, they will ask what symptoms you have, when they began, how long you experienced them, etc. After taking your history, they will examine your vulva for signs of active lichen sclerosus. Further, they may gently touch different areas of the vulva with a cotton swab to determine if there is pain. If there are both symptoms of lichen sclerosus and active signs of lichen sclerosus, your healthcare provider *may* make the diagnosis of lichen sclerosus.
Biopsies: What You Need to Know
The gold standard for lichen sclerosus diagnosis is a vulvar biopsy. Your healthcare provider may do a biopsy if:
- They want you to have absolute confirmation of the diagnosis.
- They aren’t confident in their diagnosis based on a clinical examination.
- They feel your symptoms or signs could be attributed to more than one vulvovaginal condition, and they want to make sure they get it right. (Check out differential diagnoses for lichen sclerosus here).
- There are signs of potential cancer/malignancy.

A vulvar biopsy involves taking a sample of the vulvar tissue. This is typically done via a punch biopsy. First, the doctor *may* apply a topical numbing ointment to the anesthetic injection site. Unfortunately, this doesn’t seem to be common practice. Then, they will inject you with a local anesthetic. Once the anesthetic has numbed the area, the doctor will use a sharp, circular instrument to remove a sample of tissue. This instrument removes a small, round piece of tissue, only a few millimeters across and deep. Afterward, your doctor will send the sample to pathology.
Shave biopsies are sometimes, but very rarely, used for diagnosing lichen sclerosus. This is because lichen sclerosus causes changes all the way down to the basement layer of the vulvar skin. Therefore, it is ideal for the clinician to do a punch biopsy so they can get a more comprehensive picture of what is going on. Dr. Estella Janz-Robinson notes that shave biopsies are useful for raised lesions such as skin tags. On the other hand, punch biopsies are more useful for inflammatory diseases/conditions and/or when it is important to determine the depth of the disease. This can be a conversation you have with your doctor, but note that most of the time, a punch biopsy is preferred. (Link to source).
Ideal Time to Get Biopsied
Ideally, a biopsy should be done before starting topical corticosteroids. This is because steroids are very effective at reducing inflammation. In fact, they are so good at this that they can actually obscure the histopathologic findings of your biopsied tissue sample. The best practice at the time I am writing this, according to Dr. Goldstein and Dr. Krapf, is to have patients stop using their steroids for a minimum of two to three weeks prior to biopsy. However, Dr. Andrew Goldstein has stated topical corticosteroids *may* obscure the results of a biopsy forever, making a definitive diagnosis impossible (The Centers for Vulvovaginal Disorders Lichen Sclerosus Webinar).
What Happens to My Biopsy Once It Is Sent to Pathology?
After your provider performs the biopsy, your sample will be sent to an expert pathologist for analysis. Simply put, a pathologist looks at body tissue samples to assess for disease. Additionally, your doctor will include notes to the pathologist. For example, they may note ‘Check for lichen sclerosus’ or ‘Patient presents with thickened plaques of white skin and itch’.
The Pathologist Is Looking For Four Key Features:
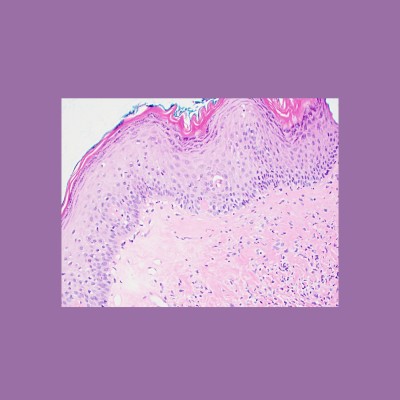
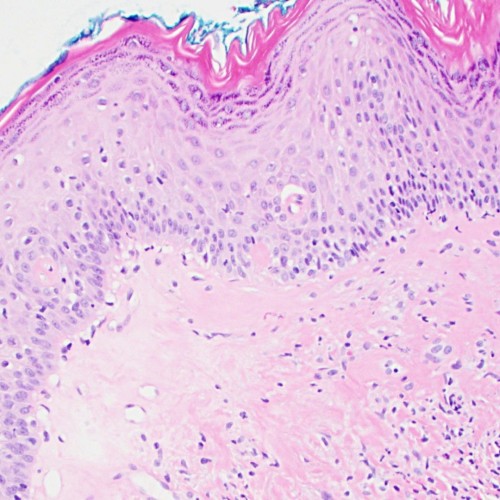
- “Hyperkeratosis of the epidermis” (aka thickening of the vulvar skin tissue, especially the mid to top layer of the skin). (The Centers for Vulvovaginal Disorders Lichen Sclerosus Webinar, 2021).
- “Epidermal atrophy with loss of rete ridges”. Let’s break down those scientific terms. If you look at a biopsy of healthy vulvar tissue, you will see ‘finger-like’ bulges between the top and middle layers of the skin. Those bulges help keep the skin together. However, with lichen sclerosus, those ‘finger-like’ bulges disappear. This makes it harder for the skin to stay together, which can result in skin tearing and blood blisters (ibid).
- “Homogenization of the collagen below the dermal-epidermal junction”. Again, let’s break down the science (ibid). Healthy vulvar tissue should have a bunch of cells. However, there aren’t many cells present in lichen sclerosus skin. Additionally, there is a lot of collagen built up. This is a part of what is responsible for the classic thick, white skin seen on vulvas with lichen sclerosus (ibid).
- “Lichenoid T-cell infiltrate near the basement membrane”. Lichen sclerosus skin will show lots of white blood cells in the bottom layer of the skin. The presence of many white blood cells means there is a lot of inflammation (ibid).
Getting Your Biopsy Results
Once the pathologist analyzes your tissue sample, they will send a report with their findings and notes to your doctor. How long it takes to get your results will vary depending on the country you live in, the backlog, etc. However, on average, it takes approximately two weeks.
After the doctor gets the results, they will have a conversation with you explaining the findings. If it is positive for lichen sclerosus, they should explain what lichen sclerosus is, your treatment plan, and answer any questions you may have.
Depending on where you live, you may get access to your report before your doctor calls to explain your results. Your results may not say lichen sclerosus per se but instead may use outdated terms such as “Lichen sclerosus et atrophicus”. Consult with your healthcare provider to confirm what the terms on your report mean.
Important Notes on Biopsies
Critically, before, during, and after the biopsy, you should be having an open conversation with your doctor. Throughout the entire process, they should explain what they are doing and why. Additionally, they should address your concerns and respect your feelings.

Conclusion
In sum, biopsies are the gold standard for lichen sclerosus diagnosis. However, a specialist can make a clinical diagnosis if there are active signs of lichen sclerosus and the symptoms match. A biopsy is typically performed via a punch biopsy. An expert pathologist will assess the tissue sample for four key indicators of lichen sclerosus and give the diagnosis if they are present.
Are You Struggling with Stress and Lichen Sclerosus?
Are you ready to learn more about how stress can impact your flares, symptoms, and ability to get into (and stay in) remission? Do you want to empower yourself with information and take active steps to reclaim your life?
If this sounds like something you need, you have to register for my Vagus Nerve and Lichen Sclerosus Workshop.
Reach Out to Me
If you want to chat with me about biopsies or Lichen Sclerosus, I can be reached at:
Instagram: @thelostlabiachronicles
Facebook: @TheLostLabiaChronicles
Email: lostlabiachronicles@gmail.com
Virtual Meetups
Do you want more support in your journey with Lichen Sclerosus? Consider joining our Lichen Sclerosus Support Virtual Meetups. We meet bi-weekly, every other Saturday from 2-4 and 7-9 pm EST. These meetups are a safe space for you to share your story, cry, celebrate, vent, ask questions, and be a part of a community of support. Click the link below to sign up!

Sign up for Lichen Sclerosus Support Virtual Meetups
Sources Cited
The Centers for Vulvovaginal Disorders Lichen Sclerosus Webinar, 2021.
“How to Perform a Vulvar Biopsy“. Welch et al, OBG Management | June 2020 | Vol. 32 No. 6.
“Vulval Biopsy” Author: Dr Estella Janz-Robinson, Resident Medical Officer, ACT Health, Canberra, Australia. Editor in Chief, Hon A/Prof Amanda Oakley, Dermatologist, Hamilton, New Zealand, October 2016.
Kirtschig, Gudula. “Lichen Sclerosus-Presentation, Diagnosis and Management.” Deutsches Arzteblatt international vol. 113,19 (2016): 337-43. doi:10.3238/arztebl.2016.0337